Pay for verified service delivery, not planned activity
Pick the program, geography, and amount. Frontline Workers deliver in their own communities, paid only for verified services. Everyone sees the results.
Frontline Workers deliver and get paid for verified services
Frontline Organizations train workers to learn new skills.
Before anyone delivers a service, they train. Workers move through comprehensive digital training and must pass a certification test before they’re cleared to deliver services in the field.
Features
Self-paced lessons
In-app assessment
AI coach
Peer practice
Supervised visits
85%of Frontline Workers moved from training to delivery
Locally Led Organizations know their communities best. Connect provides the app, verification, and payment system, while organizations bring the relationships, supervisors, and trust.
Once services are verified, the worker receives a mobile money payment to their phone. Connect charges a 20% program management fee, with remaining 80% funds going directly to the frontline.
Funders track exactly what was delivered, where, and at what cost, paying for outcomes not effort. Frontline Workers see their verified service record, earnings, and reputation grow with every visit.
Connect is live across 13 countries. Whether you’re funding a campaign, designing a program, or delivering services on the ground, let’s see how Connect can work for you.
Connect is as much a learning system as a delivery one. Here we share what’s working, what isn’t, and how the model keeps shifting in response.
Filter by Program
Filter by Activity
Insights from the field
ProgramChild Health Campaign
ActivityVerify
SourceFounders Pledge Final Report
97.5% of real workers scored cleaner than paid fakers in adversarial testing.
In adversarial testing we paid Frontline Workers to generate fake data with financial rewards for those who did best. A model trained on three data fields hit AUC 0.91, detecting 100% of fake Frontline Workers while only flagging 2.5% of real Frontline Workers as suspicious.
ProgramChild Health Campaign
ActivityVerify
SourceFounders Pledge Final Report
Map grids pushed coverage from 84% to 94%.
Without a grid, Frontline Workers cherry-picked easy houses. With a grid forcing them to go door-to-door, the hardest-to-reach children stopped being the ones who got missed.
ProgramChild Health Campaign
ActivityPay
SourceFounders Pledge Final Report
Total cost per verified visit fell 22%, from $2.20 to $1.70, as the program scaled.
That figure is Connect’s all-in cost per visit, including commodities, LLO payments, setup, and product cost. The biggest driver of the drop was setup costs falling from ~$0.40 to ~$0.10 per visit as we moved past early-stage inefficiencies. We report cost-per-verified-outcome rather than cost-per-worker-trained because it’s the number that actually matters.
ProgramChild Health Campaign
ActivityDeliver
SourceFounders Pledge Final Report
Pre-vetting didn’t predict performance. So we started contracting small.
Past reputation, team size, references, none of it told us if a partner organization would actually deliver. So we contracted small first. Of 37 partners, 24 ran trial runs. 10 underperformed. 3 were selected to scale based on their performance.
ProgramChild Health Campaign
ActivityDeliver
SourceStage 2 Report
5 of 7 partner organizations leveraged religious leaders for vaccine outreach before we asked.
Locally Led Organizations independently mobilized imams, pastors, village elders, and community-recommended Frontline Workers. The platform didn’t teach this, they already knew.
ProgramChild Health Campaign
ActivityDeliver
SourceFounders Pledge Final Report
Both partners in the Central African Republic dropped out. We now flag fragile contexts as needing in-country presence rather than remote coordination alone.
Remote coordination worked across Nigeria, Kenya, Uganda, Tanzania. It didn’t hold in the Central African Republic. Staffing turnover and connectivity issues exited both contracted partners.
ProgramKangaroo Mother Care
ActivityVerify
SourceConceptual Model
Kangaroo Mother Care 3-day visits hit 50% against a 70% goal.
If missing the window cost a worker money, we’d see suspiciously perfect compliance instead. So we treat it as a guardrail, not a payment criterion. We coach and integrate hospital discharge notifications to close the gap.
ProgramKangaroo Mother Care
ActivityVerify
SourceConceptual Model V1
Average time to first newborn visit is 6.05 days, twice our 3-day target. Only 34% reach families inside the window.
The headline 50% number understates the gap. The mean is 6.05 days. One delivery opportunity doesn’t collect hospital discharge dates at all, so 100% of those records are blank on this metric, which means the real-world bottleneck is data plumbing, not worker effort.
ProgramKangaroo Mother Care
ActivityDeliver
SourceGiveWell-shared 2-page proposal
Two partner organizations and Uganda’s Ministry of Health signed an agreement to scale to 50,000 vulnerable newborns over two years.
The Ministry is participating in working groups, quarterly reviews, and site visits, and contributing data to Uganda’s five-year national neonatal plan. The next step: government co-funding at $10-20 per case.
ProgramKangaroo Mother Care
ActivityPay
SourceConnect individual-giving blog
$60 delivers one newborn through the Kangaroo Mother Care program.
That covers partner engagement, the Kangaroo wraps, scales, thermometers, pulse oximeters, training, payment per verified case, and supervision. We picked it for our first individual-giving experiment because $60 is the smallest unit at which one donor can fund a complete intervention with verified delivery.
ProgramEarly Childhood Development
ActivityLearn
SourceECD Overview, Stage 2 Report
Passing the digital test didn’t mean passing the first real visit. So we layered supervised visits.
Workers who passed our digital test still struggled with nuanced in-home counseling. No single layer of training was sufficient. This improved with 78% of workers scoring above 80% during their first observed visits. Average performance increased from 85% to 91% in the second observed visit.
ProgramEarly Childhood Development
ActivityLearn
SourceMalawi pilot
Caregivers’ parenting attitudes were already correct. We moved knowledge +33% and observed teaching +21%.
A 50-caregiver baseline showed near-universal endorsement of responsive caregiving. Attitudes weren’t the gap. Knowledge and observed teaching practice were, and that’s where we saw movement. We doubled the visit cadence in the next round.
ProgramEarly Childhood Development
ActivityDeliver
SourceECD Overview, Stage 2 Report
Encouraging child autonomy is the hardest domain to move. 47% endline rate. We’re still working on it.
Autonomy encouragement requires consistent behavior change across many interactions, not a single coaching session. It’s the sub-domain least moved by the current visit structure. We aim to expand from 3 to 8-10 visits per child specifically to give this target more runway. We don’t know yet if it will be enough.
A note on methodology
Every Insight on this page is published in a funder report, an independent evaluation, or a public partner document.
Every entry above is a claim we have decided is honest, scoped, and worth putting on the public record. The cut is editorial. We keep what carries a number with a benchmark, what was published in a funder report or independent evaluation, and what comes with an open question we will name. We exclude headline scale numbers without context, marketing-friendly framings without source, and anything that hasn’t survived a depth page yet.
This is the complete published set. New entries are added as programs produce results that clear the editorial bar. Underlying reports are available to funders and researchers on request.
FOR FUNDERS & RESEARCHERS
Interested in seeing the numbers?
We’d be happy to share the underlying data with you. Just reach out.
Fund specific, verified service deliveries: a child vaccinated, a mother coached, a newborn attended to. Every dollar linked to a confirmed service delivery.
A Child Health Campaign is a coordinated push where Frontline Workers move household-to-household across a defined area, delivering a bundle of high-impact services to every child under five they reach. Every service is logged, photographed, and independently verified before payment.
Service 1
Vitamin A Supplementation
Vitamin A is one of the cheapest ways to save a child’s life: roughly $1 per capsule, with an estimated 4-12% reduction in under-five mortality. The hard part isn’t the capsule. It’s reaching the children. That’s what Connect campaigns are built to do.
Albendazole or Mebendazole for children with soil-transmitted helminth exposure. Routine deworming improves nutritional status, school attendance, and growth in high-prevalence areas.
Service 3
Oral Rehydration Solutions (ORS)
Distribution and caregiver coaching on ORS, one of the highest-impact, lowest-cost diarrhea responses in low-resource settings.
Service 4
Malnutrition Screening
Mid-Upper Arm Circumference (MUAC) measurement and visual assessment for wasting. Children with red or yellow readings are referred into the local treatment pathway. Data flows back to inform the next campaign cycle.
Service 5
Immunization Promotion
Caregiver counseling on routine immunization, with referral to the nearest catch-up site. Several partners independently mobilized faith and community leaders to drive coverage.
Child Health Campaigns At a glance
Stats
$1.70
Per verified visit
1M+
Verified visits
9
Countries
Countries
Central African Republic · DR Congo · Kenya · Liberia · Nigeria · Sierra Leone · Tanzania · Uganda · Zambia
Frontline Workers from Kikapu Gardens, a Locally Led Organization in Kenya, walk through their day delivering Child Health Campaign services with Connect. Trained workers visit households door-to-door, providing vitamin A, deworming, and malnutrition screening to children under five.
Hear from the organization’s staff, the workers themselves, and the families whose children received care.
Connect · Kenya · Kikapu GardensWatch
WHAT WE’VE LEARNED
The numbers behind Child Health Campaigns
Child Health Campaign is the program where most of Connect’s methodology was first validated. A few of the published findings:
ProgramChild Health Campaign
ActivityPay
SourceFounders Pledge Final Report
Total cost per verified visit fell 22%, from $2.20 to $1.70, as the program scaled.
That figure is Connect’s all-in cost per visit, including commodities, LLO payments, setup, and product cost. The biggest driver of the drop was setup costs falling from ~$0.40 to ~$0.10 per visit as we moved past early-stage inefficiencies. We report cost-per-verified-outcome rather than cost-per-worker-trained because it’s the number that actually matters.
ProgramChild Health Campaign
ActivityDeliver
SourceFounders Pledge Final Report
Pre-vetting didn’t predict performance. So we started contracting small.
Past reputation, team size, references, none of it told us if a partner organization would actually deliver. So we contracted small first. Of 37 partners, 24 ran trial runs. 10 underperformed. 3 were selected to scale based on their performance.
ProgramChild Health Campaign
ActivityDeliver
SourceStage 2 Report
5 of 7 partner organizations leveraged religious leaders for vaccine outreach before we asked.
Locally Led Organizations independently mobilized imams, pastors, village elders, and community-recommended Frontline Workers. The platform didn’t teach this, they already knew.
Let’s build one together, starting with your desired geography and budget. We’ll come back with a delivery plan, a cost-per-verified-visit estimate, and a list of frontline organizations to run with.
80% of neonatal deaths happen after discharge, at home, without follow-up. Connect KMC closes that gap with structured home visits for small and vulnerable newborns in their first 60 days, verified and paid only when confirmed.
Each home visit is a structured clinical encounter. Frontline Workers arrive with a scale, thermometer, pulse oximeter, and measuring tape. They assess weight, axillary temperature, respiratory rate, oxygen saturation, head circumference, and feeding. Danger signs trigger an automated referral before the worker leaves.
Service 1
KMC Coaching and Feeding Support
Workers deliver Kangaroo wraps and nutritional support, position the newborn skin-to-skin, and observe a breastfeed. Feeding difficulty is one of the earliest signals of clinical deterioration in small newborns. Mothers also receive emotional support. Many face stigma and isolation after a high-risk birth.
Service 2
Weight Monitoring
Calibrated scale used at every visit. Weight-for-age tracking identifies faltering growth before it becomes acute malnutrition. Workers log the reading directly into the app and flag any drop from the prior visit.
Service 3
Temperature Assessment
Axillary temperature measured at every visit. Hypothermia is the leading preventable danger sign in small and vulnerable newborns. Any reading outside the normal range triggers an immediate referral pathway in the app.
Service 4
Oxygen Saturation
Pulse oximeter reading captures respiratory status at each visit. Low saturation is an early indicator of distress before visible symptoms appear. The reading is logged alongside respiratory rate and breathing observation.
Service 5
Danger Sign Screening and Referral
Structured checklist covering convulsions, jaundice, difficulty breathing, poor feeding, hypothermia, and abnormal skin color, with automatic referral generation when any is flagged. Workers do not leave until a referral plan is confirmed with the family. Facility linkages are pre-established.
Kangaroo Mother Care At a glance
Program Stats
$60
Per newborn
5k+
Cases tracked
50K
Uganda 2-yr case target
Global Context
40%
Mortality reduction possible with KMC
<5%
Current global KMC coverage
2.3M
Neonatal deaths per year
Active Countries
EthiopiaIndiaKenyaNigeriaUganda
Partners
Uganda Ministry of HealthNama Wellness Center
PARTNER STORY · Nama Wellness Center, UGANDA
Nantume Madrine’s baby came home early.
When Nantume Madrine’s premature baby was discharged from a hospital in Mukono District, Uganda, she had almost no support. A Nama Wellness Center Frontline Worker enrolled her in Connect KMC within days. The baby thrived.
Nama Wellness Center trained 10 community health workers and reached 64 mother-baby pairs in Mukono in the first weeks of launch. Their post reads: "This is more than data. It is life, dignity, and second chances."
Two Ugandan partner organizations have now committed to delivering Connect KMC to an additional 5,000 Severely Vulnerable Newborns over the next year, expanding from Central Uganda into Eastern Uganda, with Uganda’s Ministry of Health signing an MoU targeting 50,000 Severely Vulnerable Newborns nationally over two years.
WHAT WE’VE LEARNED
The numbers behind Kangaroo Mother Care
KMC is the program where Connect first applied outcome-based payment to newborn health. A few of the published findings:
ProgramKangaroo Mother Care
ActivityVerify
SourceConceptual Model
Kangaroo Mother Care 3-day visits hit 50% against a 70% goal.
If missing the window cost a worker money, we’d see suspiciously perfect compliance instead. So we treat it as a guardrail, not a payment criterion. We coach and integrate hospital discharge notifications to close the gap.
ProgramKangaroo Mother Care
ActivityVerify
SourceConceptual Model V1
Average time to first newborn visit is 6.05 days, twice our 3-day target. Only 34% reach families inside the window.
The headline 50% number understates the gap. The mean is 6.05 days. One delivery opportunity doesn’t collect hospital discharge dates at all, so 100% of those records are blank on this metric, which means the real-world bottleneck is data plumbing, not worker effort.
ProgramKangaroo Mother Care
ActivityPay
SourceConnect individual-giving blog
$60 delivers one newborn through the Kangaroo Mother Care program.
That covers partner engagement, the Kangaroo wraps, scales, thermometers, pulse oximeters, training, payment per verified case, and supervision. We picked it for our first individual-giving experiment because $60 is the smallest unit at which one donor can fund a complete intervention with verified delivery.
$60 covers the full Connect KMC cycle for one small and vulnerable newborn: Kangaroo wraps, scales, thermometers, pulse oximeters, Frontline Worker training, payment for visits, and supervision. Every dollar is tied to a verified outcome. Individual donors, foundations, and program funders all welcome.
Home visits supporting responsive caregiving and early child development. Multiple structured visits building caregiver knowledge, observable teaching behavior, and child autonomy.
What is involved in an Early Childhood Development visit?
Each visit is a structured caregiver coaching session. Frontline Workers guide parents through responsive interaction, model talk-and-play activities, discuss developmental milestones, and practice teaching behaviors with the caregiver. The intervention targets knowledge and observable behavior.
Domain 1
Responsive Caregiving Coaching
Structured guidance on noticing and responding warmly to a child’s cues. Workers use scenario-based coaching to build the habit of responsiveness across feeding, play, and daily routines, not just during the visit itself.
Domain 2
Talk-and-Play Facilitation
Language-rich interaction and age-appropriate play activities for cognitive and language development. Workers model activities with available household materials, no kit required, and coach caregivers to continue between visits.
Domain 3
Developmental Milestone Education
Knowledge building on what children are developmentally capable of at each age, and what caregiver behavior supports progression. Caregiver knowledge of rapid development timing improved 33% in the Malawi pilot.
Domain 4
Teaching Behavior Practice
Observed teaching behavior improved 21% in the Malawi pilot. Workers do not just explain. They watch caregivers practice, give feedback, and code the quality of what they see using a structured visit checklist.
Domain 5
Encouragement of Child Autonomy
Supporting children’s exploration and independent problem-solving. This is the hardest sub-domain because it requires pattern-based behavior change across multiple interactions, not a single coaching session.
Domain 6
AI-Powered Coach Bot
An in-app AI coach built on Dimagi’s Open Chat Studio platform reinforces learning between visits. The coach runs daily: presenting practice scenarios, identifying knowledge gaps, and drilling motivational interviewing techniques like open-ended questions and reflective listening. At the end of each day it asks about how visits went and provides tailored feedback grounded in real experiences.
Early Childhood Development At a glance
Stats
150K+
Visits delivered
+33%
Knowledge gain
85%
Workers passed digital learning
Active Countries
MalawiMozambiqueNigeria
WHAT WE’VE LEARNED
The numbers behind Early Childhood Development
ECD is the program that most challenged our assumptions about what intervention design needs to target. A few of the published findings:
ProgramEarly Childhood Development
ActivityLearn
SourceMalawi pilot
Caregivers’ parenting attitudes were already correct. We moved knowledge +33% and observed teaching +21%.
A 50-caregiver baseline showed near-universal endorsement of responsive caregiving. Attitudes weren’t the gap. Knowledge and observed teaching practice were, and that’s where we saw movement. We doubled the visit cadence in the next round.
ProgramEarly Childhood Development
ActivityLearn
SourceECD Overview, Stage 2 Report
Passing the digital test didn’t mean passing the first real visit. So we layered supervised visits.
Workers who passed our digital test still struggled with nuanced in-home counseling. No single layer of training was sufficient. This improved with 78% of workers scoring above 80% during their first observed visits. Average performance increased from 85% to 91% in the second observed visit.
ProgramEarly Childhood Development
ActivityDeliver
SourceECD Overview, Stage 2 Report
Encouraging child autonomy is the hardest domain to move. 47% endline rate. We’re still working on it.
Autonomy encouragement requires consistent behavior change across many interactions, not a single coaching session. It’s the sub-domain least moved by the current visit structure. We aim to expand from 3 to 8-10 visits per child specifically to give this target more runway. We don’t know yet if it will be enough.
Interested in supporting early childhood development?
Let’s build a program together, starting with your target geography, age group, and budget. We’ll come back with a delivery plan, a cost-per-child estimate, and a partner list.
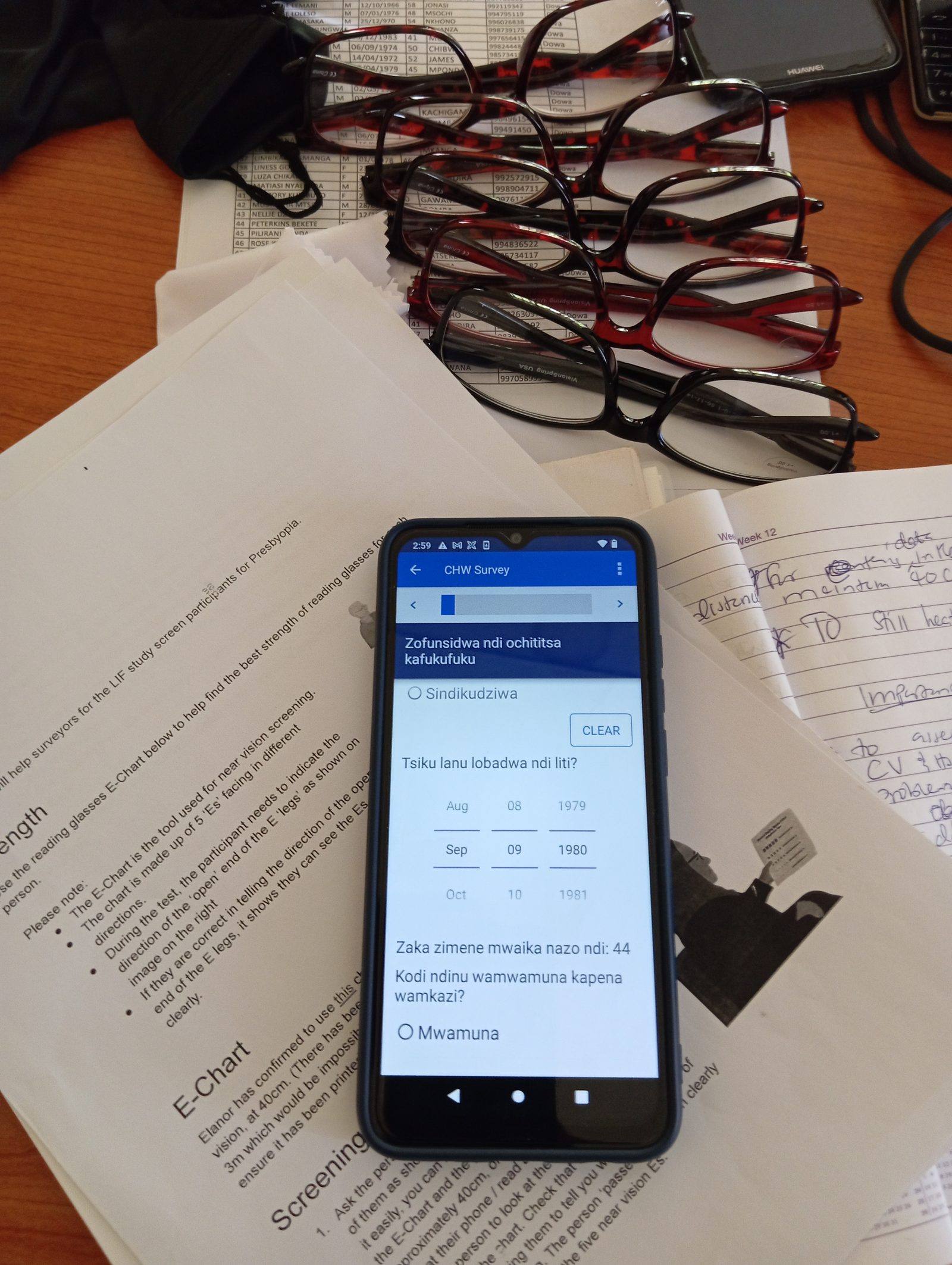
A Reading Glasses visit is a two-part encounter: near-vision screening first, then distribution. Frontline Workers screen adults aged 35 and older with a paper E-chart, identify the appropriate correction strength from five dioptre options, dispense the pair, and photograph the completed distribution for independent audit.
Component 1
Near-Vision Screening
Paper E-chart test administered door-to-door to identify presbyopia in adults aged 35 and older. Standardized distance and lighting conditions are part of the certification protocol. Pre-training test averaged 36/100; post-training averaged 93.5/100.
Component 2
Dioptre Selection
Five correction strengths available: +1.0, +1.5, +2.0, +2.5, and +3.0 dioptres. Workers test each beneficiary with the E-chart at the appropriate reading distance to identify the correct strength before dispensing.
Component 3
Reading Glasses Dispensing
Off-the-shelf reading glasses in the matched dioptre strength, handed directly to the beneficiary. Vision correction has been shown to increase work productivity up to 22% and income up to 33% for adults in visually-intensive occupations.
Component 4
Photo Verification
Every completed distribution is photographed live in the app. Photos are compared against specified criteria to ensure appropriate distribution.
Component 5
Dual-Stage Certification
Four self-paced digital modules, an 80%-threshold in-app test, then a two-day in-person practical evaluation.
PROGRAM IN ACTION · KENYA PILOT
Siaya County, Kenya: 1,239 Verified Distributions.
GlobCom, endorsed by the Siaya County Ministry of Health, deployed Community Health Promoters (CHPs) across their existing catchment areas in November–December 2024. 25 of 32 enrolled CHPs completed self-paced digital training and in-person certification before delivering services. A daily cap of 5 distributions kept incentives aligned with CHPs’ existing core health duties.
1,387 household visits. 1,239 verified distributions. The platform flagged 26 duplicate registrations and rejected 30 shortened visits before payment was processed. Workers were paid 17–32 days after service delivery. Two months post-distribution: 12 of 19 recipients confirmed they were using their glasses, for bible study, reading, and phone use.
RUN A READING GLASSES PROGRAM
Interested in scaling vision correction?
Let’s build a program together, starting with your target geography and scale. We’ll come back with a delivery plan, a cost-per-pair estimate, and a list of organizations ready to run with.
Frontline coaches support families through two proven programs: breastfeeding support, and maternal mental health care using the WHO’s Problem Management Plus approach. Six structured home visits per family, paid on verified outcomes.
Six structured home visits across two components. Each visit is delivered by a trained Frontline Worker, confirmed on the Connect platform, and paid only when verified.
COMPONENT 1 · BREASTFEEDING PROMOTION
Visits 1-2 · Antenatal
Breastfeeding Preparation
Counseling before birth on the importance of exclusive breastfeeding, what to expect in the first days, and how to prepare for early latch. Frontline Workers address misconceptions and build household support before the baby arrives.
Visits 3-4 · 0-6 Weeks
Early Breastfeeding Establishment
Workers observe a breastfeed, assess latch and positioning, and address the most common barriers to exclusive breastfeeding in the first weeks: pain, perceived low supply, and family pressure to supplement. Evidence suggests programs like this can increase exclusive breastfeeding rates by up to 48%.
Visits 5-6 · 6 Weeks-6 Months
Sustained Feeding and Complementary Transition
Support to maintain exclusive breastfeeding through six months, followed by counseling on the safe introduction of complementary foods. Workers reinforce feeding cues, responsive feeding, and appropriate meal frequency and diversity.
COMPONENT 2 · MATERNAL MENTAL HEALTH
Mental Health · PM+
Problem Management Plus Coaching
WHO’s Problem Management Plus (PM+) is a 5-session brief psychological intervention, transdiagnostic, meaning no formal diagnosis is required. It targets depression, anxiety, and stress using strategies including problem management, behavioral activation, social support strengthening, and psychoeducation. Designed specifically for delivery by trained non-professional community health volunteers, it has been validated in Randomized Controlled Trials including with women affected by gender-based violence in Kenya.
Mental Health · Wellbeing
Resilience and Emotional Support
Structured check-ins on maternal wellbeing, practical problem-solving techniques, and stress management strategies, each session using motivational interviewing and relapse prevention to build lasting change. Workers are trained to identify postpartum depression symptoms and refer when clinical support is needed, with referral pathways pre-established before first delivery.
Digital · AI Coach
AI Chatbot Reinforcement
Between visits, Frontline Workers access an AI chatbot for content reinforcement, troubleshooting, and post-session debriefs using motivational interviewing. The system also identifies workers lacking content mastery and flags them for supervisor follow-up. A potential client-facing layer for direct breastfeeding guidance is in design.
Mother Baby Wellness Piloting 2026
GiveWell awarded $320,356 in November 2024 to design and test the Mother Baby Wellness program on Connect. A 15-month design-and-pilot phase is underway, targeting approximately 2,000 mother-baby pairs across Nigeria. Data and results will be published as the pilot completes.
Nearly half of all under-five deaths happen in the first month.
Neonatal mortality is declining more slowly than post-neonatal mortality. The window immediately after birth, when most families have returned home but before postnatal clinic follow-up begins, is the single most under-supported period in the maternal and child health continuum.
The evidence for the two interventions is strong: structured breastfeeding promotion programs can increase exclusive breastfeeding rates by up to 48%. Problem Management Plus (PM+) is a WHO-endorsed brief psychological intervention shown to reduce depression and improve wellbeing in low-resource settings. Neither has been consistently delivered at scale through verified, performance-paid Frontline Workers. That is the gap MBW is designed to close.
SUPPORT MOTHER BABY WELLNESS
Interested in postnatal care at scale?
We’re actively designing the Mother Baby Wellness program. If you’re interested in co-designing, funding, or piloting, reach out. We’d like to build it with you.
Chlorine dispensers installed at communal water points, paired with door-to-door household education on safe water treatment. Diarrhea kills more children under five than malaria, and chlorination is one of the highest-evidence, lowest-cost ways to stop it.
A chlorine dispenser program combines physical infrastructure at the point of water collection with frontline-delivered household education. Workers install and maintain dispensers, train communities on correct use, conduct door-to-door counseling on safe water storage, and monitor adoption and usage. Every visit is logged and verified through the Connect platform.
Service 1
Dispenser Installation
Chlorine dispensers are mounted directly at communal water points (boreholes, hand pumps, and collection taps), so households can self-dispense chlorine into their containers as they collect water. Installation is coordinated with local health authorities and water point operators.
Service 2
Household Education
Door-to-door visits to every household in the program area. Frontline Workers demonstrate correct chlorine dosing, explain how chlorinated water prevents diarrhea, and address common household-level barriers to adoption, including taste concerns, confusion about dosage, and beliefs about water safety.
Service 3
Safe Water Storage Counseling
Guidance on storing treated water safely at home (covered containers, dedicated water vessels, hand-washing at water collection) to prevent recontamination after chlorination. Chlorinated water remains safe for up to 72 hours when stored correctly.
Service 4
Community Mobilization
Engaging community leaders, water point operators, and faith networks to drive adoption. Local organizations with existing community relationships recruit the Frontline Workers who deliver household education, the same locally led model used across every Connect program.
Service 5
Usage Monitoring and Refill
Regular checks on dispenser stock levels and usage rates. Empty dispensers are refilled; broken units are reported for repair. Monitoring data is captured in the Connect app, giving program managers visibility on coverage and adoption across the deployment area.
Chlorine Dispenser Launching 2026
GiveWell awarded a $1M grant in January 2026 to launch chlorine dispenser installation and household education across Nigeria. The program is part of GiveWell’s $19.7M Safe Water portfolio, 18 grants to 12+ organizations delivering safe water across West and East Africa. Data and findings will be published as the program launches.
Chlorination is one of the most robustly evidenced low-cost water interventions in global health. Point-of-collection dispensers (liquid chlorine mounted directly at hand pumps and communal water points) consistently outperform household-level filters and sachets on adoption, because the behavior change is smaller: chlorinate at the tap, not at home.
Evidence Action’s Dispensers for Safe Water program, the model Dimagi’s program is informed by, has reached over 5 million people across Kenya, Uganda, and Malawi. GiveWell’s Safe Water portfolio, which now includes Dimagi, projects 2,000+ deaths averted across 18 active grants, mostly in children under five. The Connect platform adds verified household education delivery on top of the physical dispenser infrastructure.
Technical assistance for Connect’s program is provided by Evidence Action. Baseline and endline surveys are conducted by independent external firms. Chlorine has limited effectiveness against Cryptosporidium; the program targets bacterial and viral pathogens, which account for the majority of diarrheal disease burden in the target geographies.
SUPPORT CHLORINE DISPENSER
Interested in safe water at scale?
We’re launching the Chlorine Dispenser program in Nigeria in 2026. If you’re interested in co-funding, designing, or expanding to additional geographies, reach out.
Depression affects over 280 million people, yet fewer than 25% in low- and middle-income countries ever receive care. Connect’s Mental Health program trains local facilitators to run structured weekly group therapy, with every session app-guided, verified, and paid only when confirmed.
From facilitator training to verified group session.
Connect applies its Learn-Deliver-Verify-Pay model to group therapy. Locally Led Organizations recruit and manage facilitators, who receive digital training and then run structured weekly group sessions, tracked session by session, paid per verified completion.
Learn
Facilitator Training & Certification
Frontline Worker facilitators complete digital training on their assigned protocol: IPT-G or gPM+. The IPT-G curriculum runs approximately 35 hours; facilitators must pass in-app certification before being assigned groups. Training covers how to run sessions, track participant wellbeing using validated tools like the PHQ-9, and manage safety referrals.
Deliver
Weekly Group Sessions
Facilitators run structured weekly sessions with groups of 6-8 participants. IPT-G runs 8 sessions per intervention; gPM+ runs 5 weekly sessions. The Connect app guides the facilitator through each session, providing step-by-step prompts, counselling scripts, and structured activities. Each facilitator manages up to 4 concurrent groups. Locally Led Organizations assign cases, manage rosters, and supervise facilitators.
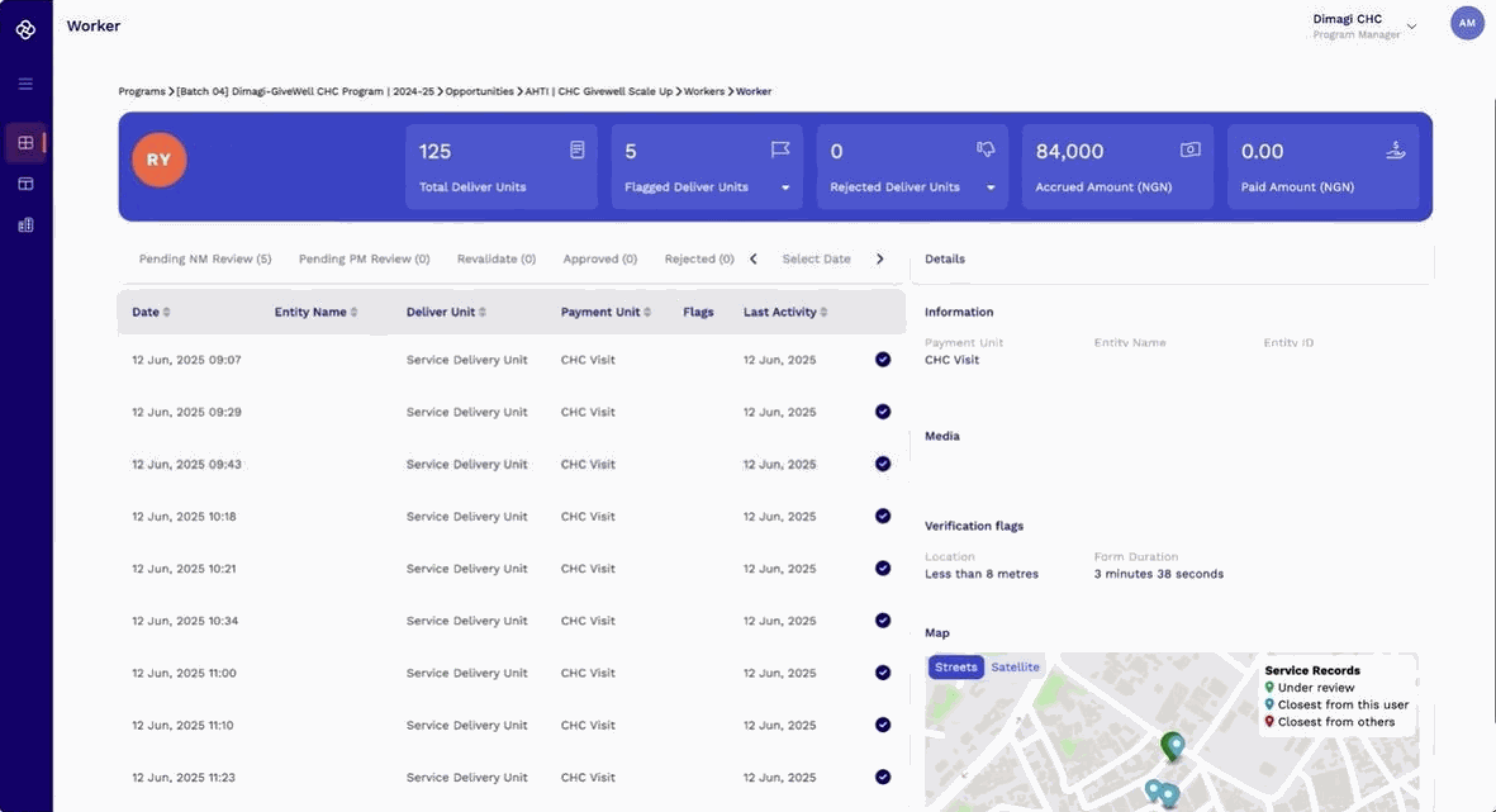
Verify
Session-by-Session Verification
Dimagi runs verification algorithms on each submitted session: GPS-based location checks, session duration (flagging sessions that are too short), and requirements that data be entered during the session itself. Claims that fail verification are rejected, and the partner organization is told why.
Pay
Pay per Verified Session
Facilitators are paid per confirmed, verified session, not per training completed or group enrolled. Locally Led Organizations receive payment after Dimagi’s verification algorithms clear each session’s data. Scores are tracked at midline and endline to monitor participant outcomes alongside delivery metrics.
Group Therapy at $25 per person treated.
Three self-funded validation pilots achieved $50 per person treated. Connect is now working with existing LLO partners to drive that cost below $25, unlocking 40,000 people treated for every $1M of funding.
Program Model
$25
Target cost per person treated
40k
People treated per $1M
655+
Women and girls treated, Nama pilot
3+
Validation pilots completed
Countries
UgandaEthiopia
Partners
Nama WellnessWorld Vision
PROGRAM IN ACTION
Pilot partners delivering group therapy at scale.
Three Locally Led Organizations have piloted group therapy and validated the model. Each brings local trust, clinical backing, and a pathway to government integration.
Uganda · IPT-G
Nama Wellness Center
Introduced IPT-G in 2021, treating depression and anxiety in 655 women and girls to date. Connect’s IPT-G app supported the initial pilot of 50 clients. Nama, in collaboration with Uganda’s Ministry of Health, is scaling to three districts, targeting 1,200 women and girls.
Uganda · IPT-G
Komo Learning Centres
Worked with locally hired facilitators to deliver school-based IPT-G sessions for over 50 children under the age of 18. Backed by Uganda’s Ministry of Education, demonstrating the model’s adaptability beyond adult clinical populations.
Ethiopia · gPM+
World Vision Ethiopia
Building on the USAID-funded SPIR II program in Tigray, where the target population exceeds 80,000, WVE deployed 120 Frontline Workers across a 5-week gPM+ pilot, running 3–4 groups each and supporting over 2,000 individuals. Backed by Ethiopia’s Ministry of Health.
FUND GROUP THERAPY
The most cost-effective mental health program we know of.
If you’re interested in funding sessions, co-designing the program, or bringing it to a new context, reach out.
Turns Frontline Workers into a rapid research network. Stakeholders submit questions, an AI chatbot interviews workers in-app, and Dimagi delivers transcripts, translations, and summaries within two weeks. Workers opt in and are paid per quality interview.
Each interview round takes approximately two weeks, end to end, from question development to completed analysis. Stakeholders get transcripts, English translations where needed, and AI-generated summaries. Workers are paid per quality response, and only the best continue to be offered interviews.
Step 1
Stakeholder Submits Questions
A stakeholder provides a set of questions to Dimagi. Questions are programmed into the AI chatbot, along with probing follow-ups.
Step 2
AI Chatbot Interviews Frontline Workers
Workers opt in through Connect’s WhatsApp-like in-app messaging. The AI chatbot, built on Dimagi’s Open Chat Studio, conducts the interview, probes for clarity, and follows up on incomplete answers. Operates in Hausa and other low-resource languages.
Step 3
Quality Rating and Payment
Responses are rated by AI and human labeling for clarity and completeness. Workers who deliver higher-quality responses continue to be offered paid interviews.
Step 4
Transcripts, Translations, and Summaries Delivered
Dimagi delivers full interview transcripts, English translations where needed, and AI-generated summaries to the stakeholder, within two weeks of question submission. Faster and cheaper than in-person qualitative research at comparable scale.
Connect Interview Piloting in Nigeria 2026
GiveWell awarded grant to develop and pilot Connect Interview over 6 months in Nigeria. The program will run 20 interview rounds, targeting 5,000 quality interviews from at least 1,500 Frontline Workers, averaging 250 participating workers per round.
Program Scale
5,000
Target quality interviews
1,500+
Target Frontline Workers
20
Interview rounds over 12 months
Countries
Nigeria
Funders
GiveWell
WHY IT MATTERS
Frontline Workers are the closest thing to ground truth.
Frontline Workers are embedded in the communities where development programs operate. They see what program data misses: what caregivers actually believe, what barriers look like at the household level, what’s changing and what isn’t. Getting that signal has historically required expensive in-person qualitative research: slow, hard to repeat, and difficult to scale.
Connect Interview makes that signal accessible on demand. Stakeholders can query a standing network of verified Frontline Workers in two weeks, in low-resource languages, at a fraction of the cost of traditional qualitative fieldwork. And because workers are paid for quality, not just participation, the answers are worth something.
RUN AN INTERVIEW ROUND
Questions you need answered from the frontlines?
Connect Interview is piloting in Nigeria in 2026. If you’re interested in running an interview round or co-designing the program, reach out.
Frontline Workers, digitally trained and app-guided, deliver home-based malnutrition treatment with Ready-to-Use Therapeutic Food (RUTF). Every visit is verified with GPS, timestamps, and photos.
Connect builds on WHO’s updated 2023 guidelines, which recognize that community health workers can deliver high-quality SAM treatment when properly trained and supervised. Every step is digitally guided, verified, and paid only when completed correctly.
Step 1
Digital Training & Certification
Frontline Workers complete self-paced, offline digital training on WHO SAM guidelines before delivering any care, covering MUAC screening, SAM diagnosis, RUTF dosing, counselling, and danger-sign recognition. Workers must pass in-app certification before they are assigned cases.
Step 2
MUAC Screening & Case Identification
Workers use mid-upper arm circumference (MUAC) to screen children aged 6–59 months in the community. Cases of uncomplicated SAM are identified and assigned to a Frontline Worker by a supervising nurse. Children with danger signs or complicated SAM are referred to a health facility.
Step 3
Guided Home Visits
At each home visit, the Connect app guides the worker through the full protocol: RUTF dosing calculation, counselling on feeding and hygiene, weight recording, and danger-sign checks. Decision support is built in. Workers are prompted when dosing adjustments or referrals are needed.
Step 4
Nurse-Led LLO Oversight
Locally Led Organizations (LLOs) employ trained nurses who assign cases, supervise Frontline Workers, manage RUTF supply chains, and coordinate referrals. LLOs receive start-up funding and pay-per-verified-service contracts, aligning incentives with quality delivery and minimising leakage.
Step 5
Digital Verification & Payment
Every visit is verified with GPS, timestamps, and photos before triggering payment. Workers are paid only for confirmed, quality visits. The platform collects continuous data on service delivery, child outcomes, and costs, enabling rigorous monitoring and rapid course correction.
18-Month Pilot in Northern Nigeria
The Children’s Investment Fund Foundation (CIFF) is funding an 18-month pilot to develop and validate a scalable, low-cost model for community-based SAM treatment in northern Nigeria, with a target cost of $30 per case, excluding RUTF.
Program Model
$30
Target cost per case (excl. RUTF)
18 mo.
Pilot duration
6–59
Months, target age range
Countries
Nigeria
Funders
Children’s Investment Fund Foundation
WHY IT MATTERS
Distance and cost shouldn’t decide who gets treated.
Severe malnutrition affects tens of millions of children globally and is a leading cause of child mortality, yet most treatment requires repeated trips to a health facility, which many families cannot manage. WHO’s updated 2023 guidelines recognize that community health workers can correctly screen, diagnose, and treat uncomplicated SAM when given adequate training, supervision, and motivation.
Connect brings together digital certification, guided delivery, nurse-led oversight, and pay-per-verified-visit to make that possible at scale. The 18-month CIFF-funded pilot in northern Nigeria will test whether this model can deliver high-quality care at $30 per case, and demonstrate a replicable blueprint for expanding SAM treatment beyond health facilities.
RUN A THERAPEUTIC FOOD PROGRAM
Bring malnutrition treatment home.
If you’re interested in running a therapeutic food program or co-funding the model, reach out.
A GPS-navigated household survey method that uses satellite building footprints as the sampling frame, no household list required. Developed by IDinsight, deployed with Frontline Workers as enumerators.
Rooftop Sampling uses Google Open Buildings (1.8 billion structures) or Microsoft Building Footprints as a sampling frame, replacing the household lists that traditional surveys require. Enumerators navigate directly to GPS coordinates on their phone, no paper maps needed.
Step 1
Download Building Data
Building footprints are downloaded from Google Open Buildings or Microsoft Building Footprints for the target geography. These satellite-derived datasets cover over 1.8 billion structures globally and require no in-country household list or census frame.
Step 2
Filter Buildings
Buildings are filtered by confidence score and minimum roof size to eliminate small structures unlikely to be residential. The result is a clean sampling frame of plausible households, without a single field visit.
Step 3
Sample Buildings
A random or systematic sample is drawn from the filtered frame. In the Nigeria pilot, each enumerator received 40 GPS points organized into 5 clusters of 8 buildings, clustered to minimize travel time while maintaining geographic spread.
Step 4
Navigate to GPS Coordinates
Enumerators navigate to sampled GPS points using their phone. In the Nigeria pilot, 80% arrived within 15m of the target building, and 98% of pins led to inhabited homes.
Step 5
Survey the Household
At the doorstep, enumerators conduct the household survey. In the pilot, Frontline Workers with no prior survey experience served as enumerators, receiving GPS navigation training and supervision. The survey captured vaccination coverage, child health status, and other program indicators.
Nigeria Pilot 3 States, 996 Households
The pilot covered 5 wards across Sokoto, Gombe, and Borno states, with approximately 200 households per ward, 1,846 children under five enumerated. Frontline Workers handled all fieldwork as enumerators with no prior survey experience.
Pilot Scale
996
Households surveyed
1,846
Children under five
5
Wards across 3 states
98%
Of GPS pins led to inhabited homes
Countries
Nigeria
INDEPENDENT COVERAGE MEASUREMENT
Need to know what actually happened in the field?
Rooftop Sampling provides a satellite-derived, GPS-navigated alternative to traditional household surveys: no household list required, Frontline Workers as enumerators. Reach out to explore a coverage validation study.
The platform frontline organizations have been waiting for.
Hundreds of frontline organizations are already delivering services and getting paid for verified work through Connect. See why organizations love Connect, and join the network today.
Connect runs inside the CommCare app, which is what you’ll install. Pick up real, verified work in your community. Train on your phone. Deliver visits. Get paid by mobile money the moment your work is verified.
Self-paced training in your language
Paid per verified visit, no middlemen
See your earnings as you work
Android only · Available where Connect programs are running
Funders can’t verify what reaches communities. Frontline Workers deliver results no one tracks. Two challenges. One missing link.
Two challenges, one missing link
Funders
The money moves. The results don’t.
Billions flow into global development every year, yet funders still can’t see where the money goes or what reaches communities. Programs lean on the same implementers, reach is shaped by logistics instead of need, and payment is tied to planned activity, not verified delivery.
Only10%
of US foreign assistance reaches a local organization directly
The people who could deliver are invisible to the system.
Trusted, capable local organizations are already embedded in the communities that need them most. But the old model locks them out: funding flows to a single implementer, and the hard-to-reach communities they serve get written off as too costly.
6 Million
women delivering frontline health services globally are unpaid or underpaid
Select an existing program or country, or launch a new one
Set delivery targets and quality standards
Pay only for verified delivery, as low as $1.50 / service
You see verified services delivered
Frontline Workers deliver verified services in their own communities.
Frontline workers paid for every verified service
GPS + photo verification built in
Rapid deployment in as few as 10 days
Frontline Organizations see verified services delivered
WHAT’S DIFFERENT
A new model for global development.
For decades, funders have paid for planned activity and hoped it added up. Connect changes the model to pay for work delivered, not work promised.
Traditional Global Development Model
The Connect wayNew model
Sourcing & Cost
Bet on a single organization with fixed pricing and no competition. High overhead, limited provider choice.
A marketplace of vetted local organizations. Competitive pricing, funding stays in-country, no single-vendor dependency.
Reach
Geography is set by your implementer’s logistics, not by where the need is. Hard-to-reach populations stay hard to reach.
Deploy in any community in the world. Local organizations are already embedded where the need is strongest.
Accountability
Trust the implementer to self-report, pay for costly third-party audits, and wait until program end to see what was delivered.
The platform independently verifies every service, and you see each one the moment it’s confirmed. Real data from day one, not a final report.
Payment
Pay for self-reported activity, be it workshops held, plans filled, or reports submitted.
Pay for delivery. Every service provided to a real person, household, or site, verified before payment.
THE ORIGINAL IDEA
The Origins of Connect.
Conceived in 2022, Connect draws on Dimagi’s 20 years of frontline expertise and a digital platform serving more than 200,000 frontline workers globally. The initiative launched with a $25 million anchor investment from the Steele Foundation for Hope.
SEE IT IN ACTION
Connect has delivered 1.5 million verified services.
See how it works, explore active programs, or get in touch to fund an intervention.
Release notes for the Connect platform, published with each major update to the mobile app and web tools.
Release Notes: CommCare Mobile v2.63
Planned Release: Audience: Connect users
New Features: CHC RCT
The new functionalities coming out in 2.63 are related to the new Microplanning, Auditing, and Verification workflows for the CHC RCT work, mainly around Tasking: Tasks are corrective actions assigned to Frontline Workers when their performance falls below certain thresholds identified during the Auditing process. These tasks block service delivery work until they are completed.
1. Opportunity Tile updates for Tasking
The Opportunity Tile now visually indicates when additional delivery progress is blocked due to pending Re-Learn tasks. When you have incomplete Re-Learn modules, a warning message appears on both the Delivery Progress and App Home Page, distinctly separate from any error messages. After completing the required Re-Learn content, a green confirmation message is displayed for an extended period to clearly show that delivery activities can continue.
2. Push Notifications for Tasking and Work Area Assignments
When a Program Manager assigns a re-learn task to a Connect Worker (Frontline Worker), the Frontline Worker receives a push notification on their mobile device with a message indicating that a relearning task has been assigned and must be completed before continuing Delivery activities.
When a Frontline Worker’s work area assignments change, the Frontline Worker receives a notification on their mobile device.
Enhancements and Optimizations
1. PersonalID Backup Code Page Improvements
The Backup Code page now features the familiar 6-box input from the OTP page for entering your backup code. Error messages about code length have been removed, as the interface guides you to complete all six boxes before enabling the Continue button. During new account registration, you will also see a message reminding you to memorize your backup code.
2. Enhanced Tracking for OTP Requests on Manual OTP Generation
The otp_requested analytics event now captures detailed information about manual OTP generation attempts. When a user requests or verifies an OTP, the event logs whether the action succeeded or failed, specifies the type of event (request or verify), identifies the method used (Firebase or Personal ID), and records the reason for any failure. This richer event data allows for a clearer breakdown of OTP request outcomes and user experience with OTP flows.
3. Improved Country Code Auto-Population
The country code in the PersonalID Phone page now prioritizes the user’s SIM card or network country code when available. If neither is detected, the country code falls back to the device’s configured Locale as before.
4. Locale-Friendly Date Formatting
Dates in the Connect user interface now automatically adjust to match your device’s locale settings, using a consistent and familiar date style regardless of region. All date strings throughout Connect are displayed using your local date format, replacing previously hard-coded formats.
5. Preparation for Verification Flags to Rules
The "Pending" status has been hidden from forms across the mobile app when the user has no "Pending" forms. All references to the "Pending" filter, including in visit and other relevant lists, have been hidden from the user interface if the user has no "Pending" forms.
Bug fixes
1. OTP Screen Messaging Updates
Previously, the error message shown when too many OTP requests were made was "You entered the incorrect 6-digit One Time Passcode too many times. Please try again later". It now correctly states: "You have made too many attempts to send OTP. Please wait and try again whenever the resend button is visible." The messaging on the OTP screen has also been updated to display your masked phone number, for example: "We attempted to send an SMS to your phone number ending with 1423." Additionally, the "Change" button has been relabeled to "Change Number."
CommCare Mobile v2.62 introduces a major redesign of the Connect Landing Page to improve the design, functionality, and end-to-end flow of opportunities. Key enhancements focus on user experience and information delivery, including the addition of Hausa language support, updated push notifications for instant assessment results (pass/fail), and a streamlined payment notification system. The release also features enhanced geospatial navigation for frontline workers, providing more accurate mapping and clearer visual cues within their target areas, alongside several key bug fixes
1. Landing Page Redesign
The Connect Landing Page has been redesigned to improve the design, functionality, and process flow of opportunities within the Connect app, end-to-end.
Key updates:
Updated opportunity card: Refreshed card design for clearer at-a-glance information
Progress indicator: A new visual indicator tracks your progress through an opportunity
Opportunity states: Improved handling and display of different opportunity states
Updated Learn/Delivery overview page: A refreshed overview experience for Learn and Delivery workflows
Enhancements & Improvements
1. Hausa Language Support
The app is now available in Hausa, with translated UI text throughout the platform.
2. Assessment Result Push Notification
After completing a Learn assessment, you will now receive a push notification as soon as your results are scored, indicating whether you have passed or failed. Tapping the notification takes you directly to the Job Status page so you can review your assessment outcome immediately.
3. Updated Payment Push Notification Behavior
The push notification received when you are paid for an opportunity has been updated. Key changes:
The notification now displays the message: "You have received a payment for [opportunity name] Opportunity, see how much!"
The Yes/No response options have been removed
Tapping the notification takes you directly to the Payments tab on the Delivery Status page
4. Enhanced Geospatial Navigation in CommCare
The geospatial feature in CommCare now provides improved navigation for frontline workers within their target areas. This update includes:
More accurate mapping
Clearer visual cues for boundaries and key locations
Better understanding of areas relevant to your assigned work
Bug Fixes
1. Fingerprint Configuration Error Message Update
When configuring a fingerprint during registration, you will no longer see an erroneous error message after returning from the setup process. The page now correctly reflects your updated status and prompts you with the appropriate next action. A unit test has been added to ensure this behavior remains consistent going forward.
2. Payment Tab Display Update
The payment tab now retains its correct height when switching between tabs. All payment entries remain fully visible, and the screen no longer resizes to match the height of the progress tab.
3. Automatic Navigation After App Installation
After installing a new app from the App Manager, you are now directed to the Login page with the newly installed app loaded by default. Previously, users were returned to the App Manager rather than being taken directly to the app's login experience.
The 2.61 release of the Connect mobile app introduces several new features, enhancements, and bug fixes designed to improve usability, task tracking, and overall user experience. This release includes a central Notification History, Work History with digital Credentials, improved PersonalID signup flow, and updated error messaging across the app.
1. Push Notifications and Notification History
We’ve improved push notifications to make them more reliable, even if the user doesn’t have internet at the time.
Key updates:
Notification History page: Users can now refer back to all Connect platform notifications at any time.
Types of notifications included:
New Opportunities
Reminders to resume learning
Reminders to resume delivery tasks / perform delivery visits
New payments
Centralized access: Previously, notification history could only be seen in the device’s notifications tray. Now, users can access it directly via:
Sidebar menu
Notification bell icon in the title bar
Quick navigation: Tapping any item in Notification History takes the user directly to the relevant task or page.
No changes to existing notifications: Timing, content, and configuration of Push Notifications or PersonalID messages for Connect Opportunities remain the same.
2. Work History & Digital Credentials
Workers with a configured PersonalID can now earn digital badges (Credentials) for completed delivery work.
Details for workers:
View earned badges in a new Work History page.
Receive push notifications when a new Credential is awarded.
Details for PMs:
PMs can configure preset thresholds for awarding Credentials in the Edit Opportunity menu.
New and existing Opportunities default to not issuing Credentials.
Enabling Credentials on existing Opportunities backfills previously earned badges.
Future enhancements:
Credentials for Learn modules
Pending or "not yet earned" badge views
Credentials for CommCareHQ activities
Custom delivery thresholds
Enhancements & Improvements
1. Sidebar Menu Behavior After PersonalID Signup
Sidebar automatically opens during the first session after PersonalID registration.
On subsequent sessions, it remains collapsed unless manually expanded.
2. Location Status Indicator on PersonalID Signup
During PersonalID signup, the app now provides clear messages about device location:
"Trying to get location…" while retrieving location
"Location Captured" once location is successfully acquired
If the location cannot be obtained, an error message explains the requirement and the Continue button remains disabled until resolved
3. Sign In / Register Button
Updated from a link to a button in the sidebar for better visibility and alignment with the app’s styling.
4. Completed Learn Task Banner
Learn tasks that have already been completed now display a green success banner instead of the previous red banner.
5. Improved Error Messaging
Error messages across the app have been updated for clearer language and guidance.
Many messages now include actionable next steps or updated links to relevant actions.
Bug Fixes
1. Unconfigured PersonalID/Connect Access
If a user opens PersonalID/Connect from a push notification without a configured account, a clear error message now appears prompting setup.
Users are redirected to the Setup/Login page instead of experiencing a crash.
2. Messaging Option Visibility
The Messaging menu item now appears immediately in the sidebar after signing in with PersonalID, if messaging channels exist.
Previously, it only appeared after navigating away and returning to the start screen.
Release Notes: CommCare Mobile v2.60
Planned Release: October 20, 2025 Audience: Connect users External documentation:
We’ve made several updates to improve your experience using the mobile app.
This release includes design enhancements, workflow improvements, and important bug fixes to make things run more smoothly.
Highlights at a glance
Messages are now accessed through the side navigation menu, with a new unread indicator
Android 15 users will see a refreshed edge-to-edge UI on key screens
The app is now locked to portrait mode to prevent download errors
Duplicate account creation using the same phone number is no longer allowed
Sign-up process improved with better OTP delivery handling
Clearer error messages for failed opportunity claims
Enhancements and Improvements
Easier Access to Messages
Messages have moved from the top bar to the side navigation menu.
An unread message indicator (dot) now appears when you have new messages.
This update streamlines navigation and helps you stay on top of communications.
Updated Design for Android 15
The Connect and PersonalID screens now support Android 15’s edge-to-edge display.
Content now extends behind the system bars, providing a cleaner and more modern experience aligned with the latest Android standards.
Portrait Mode Only
To prevent download issues caused by screen rotation, the app is now temporarily locked to portrait orientation.
This change ensures stable downloads while we work on a permanent fix.
Remove Ability to Create New Accounts with Existing Phone Numbers
Users can no longer create multiple accounts using the same phone number.
This prevents data and progress loss and ensures each account remains properly linked.
Improved OTP Sign-Up Reliability
The sign-up process via PersonalID is now more robust.
If sending the OTP fails during sign-up, the app will now automatically try a different service (Twilio). The message format from Twilio may look slightly different, but functionality works the same.
Bug Fixes: Clearer Error Messages for Failed Opportunity Claims
If a claim fails (e.g. because an opportunity is full or the budget is exhausted), the app now displays a clear message explaining the reason.
This helps users understand the issue and what to do next.
Overview
This release introduces significant updates, including the merge of all Connect Code into the mainline CommCare code and a new side menu in PersonalID to improve navigation. These changes will impact onboarding and training.
Beta Program No Longer Required
All Connect features are now merged into the mainline CommCare codebase.
Users no longer need to subscribe to the CommCare Beta program to access Connect functionality.
Updating the CommCare app as usual will move users from the Beta channel to the 2.59 release.
Frontline Workers should not be directed to sign up for the Beta during onboarding going forward.
NOTE: The 2.59 mainline release will roll out in phases over the first week (Aug 25, 2025 to ) During this time, beta users can continue to use the beta version. After one week, once the mainline release is fully deployed (100% users), the Beta Program will no longer be available. Connect users will no longer need to sign up for the beta, the latest version will be available by default.
New Side Menu in PersonalID
Access & Availability
A side menu is added to PersonalID to streamline navigation, accessible via a hamburger icon (≡) in the upper left corner of the app.
The side menu can appear on the Setup, Login, and App Home pages:
Always available on the Setup page.
Available on Login and App Home pages only if a PersonalID is configured on the device.
Once enabled on the Login page, it remains available even if the user "forgets" their PersonalID.
Side Menu States
Logged out State
Option to "Sign in / Register"
After you complete the PersonalID signup flow, you will be returned to the setup page.
About CommCare in the footer and app version
Logged in state:
Opportunities will be displayed on the side menu if pre-invited or if you have existing opportunities
"CommCare Apps" menu item is included on the side menu
If you have no CommCare apps installed the "CommCare Apps" menu item will not be shown
The CommCare app you last used (the "seated app") will be highlighted on the Login or Home screen.
If user has PersonalID messaging channels, "Messaging" menu item is shown
Opportunities Access
Users pre-registered to an Opportunity can select "Opportunities" from the side menu to access their Opportunity list.
Non-pre-registered users can:
Open the 3-dot menu on the Setup page
Select "Check for Opportunities"
If available, the Connect menu appears to navigate to Opportunities
Otherwise if no Opportunities are available, users see a "Try again later" message.
Additional Side Menu Details
The app version is displayed at the bottom of the side menu.
After signing in with PersonalID, users’ photo and name appear in the side menu
Analytical events added when the menu is opened and when a menu item is selected
🚀 Release Notes: Introducing PersonalID: Biometric Login for CommCare
PersonalID is a new secure login method for CommCare mobile users that leverages the phone’s built-in biometrics (like fingerprints) to provide fast and secure access to all CommCare apps on a device, no password typing required.
With PersonalID, users can log into multiple project spaces using a single, universal ID tied to their personal phone number.
🌟 Key Benefits
Streamlined Access: Log in faster using fingerprint, no need to remember or enter passwords.
Cross-App Authentication: One PersonalID grants access across all CommCare applications on the device.
Device-Based Security: Biometric data is never stored or collected by CommCare, authentication happens using native phone tools.
Offline Access: Once set up, PersonalID can be used without internet connectivity.
👤 Who Should Use It?
This feature is currently in limited release for select Connect projects.
Dimagi does not yet recommend general use of PersonalID unless:
You're part of a Connect deployment, or
A Dimagi point of contact has advised you to use it.
A general availability (GA) rollout is expected later in 2025.
🛠️ How It Works
Setup Steps:
Open CommCare Android and select "Sign up for PersonalID" from the 3-dot menu.
Enter and verify your personal phone number via a One-Time Passcode (OTP).
Configure your fingerprint on the device.
Provide your full name, create a 6-digit Backup Code, and take a profile photo.
Once complete, you'll be able to log in using your phone’s biometric prompt.
Login Experience:
Unlock your PersonalID using your fingerprint
Access CommCare apps linked to your PersonalID, no separate passwords required.
⚠️ Important Notes
A backup code is required to recover your PersonalID on a new device or reinstall.
Users must have their own phone number and device for PersonalID.
After 3 failed attempts to enter a backup code, the PersonalID will be locked and must be recreated.
Biometric authentication must be set up on the phone before PersonalID can be enabled.
📌 Known Limitations
Currently limited to select Connect projects.
Not supported for shared devices or users without personal phone numbers.
Cannot be used on devices that do not support biometrics.
🔜 Coming Soon
In late 2025, PersonalID will become available to all CommCare users. At that time, we’ll encourage all users with personal phones to switch to PersonalID for a faster, more secure experience.
CCC Web UI released on 30 May 2025
🚀 Overview
We are excited to announce the launch of the revamped CCC Web UI, designed to improve user experience and interface clarity for both internal Dimagi Program team members and external users, including Network Managers and locally led organizations.
This release is a UI/UX refresh only, all existing functionality remains intact. However, users will benefit from a richer set of operational metrics, enabling deeper insights and improved tracking of CCC activities.
✨ What’s New
Modernized User Interface: A cleaner, more intuitive layout for improved navigation and ease of use.
Enhanced User Experience: Streamlined workflows that make day-to-day interactions more efficient.
Expanded Metrics Dashboard: Access to new operational metrics for better monitoring and decision-making.
🧭 Rollout Plan
The upgrade will be rolled out universally, to all users currently on CCC will be migrated to the new UI at the same time.
Internal teams onboarded with the staging environment and did an initial review of the new UI.
We are actively monitoring feedback and questions over the next 2 weeks. Please submit any issues or questions on this form for an expedited response.
Self-Onboarding: The new UI is designed to be intuitive. Users are encouraged to explore and self-onboard.
Task Guide for Network Managers with Video Tutorials: A task guide is available here, including video tutorials and a glossary of terms.
As there are a lot of new metrics and numbers in the new UI, users may initially have questions on how to reconcile them across different parts of the UI. There is guidance available here before you reach out to the tech team through the support process
Beta APK 468051 released on 7 April 2025
Fixed scrolling issues on the mobile "Job Status" page. The scrolling issue disabled the user from scrolling all the way down to view the progress corresponding to different payment units
Fixed the information displayed on the "Job Status" page corresponding to different payment units. The "Remaining" section within each payment unit now shows the exact no. of approved visits a user needs to do within the number of days left for the opportunity to end. Also, the progress bar shows progress as each approved visit is executed by the mobile worker.
CCC Web release on 4 April 2025
With this change, a Connect web app user won't be allowed to invite a mobile worker to the opportunity as long as the opportunity setup is not complete. This further ensures a mobile worker doesn't interact with an incomplete opportunity and experiences app crashes
The PM can now add additional deliver units to a an app and make it visible within a payment unit by using the sync button below:
Better error handling to prevent 500 errors
Beta APK 468048 released on 2 April 2025
Fixed a P1 bug unintentionally introduced as part of beta release 468047. This issue was faced by multiple users wherein the users were unable to continue with delivery. The opportunity showed incorrectly as ended, even though the end date was in future